
The cornerstone of assisted reproduction. From ovarian stimulation through embryo transfer, every step with care.
In Vitro Fertilization (IVF) refers to the whole process by which eggs (oocytes) are stimulated to be mature, then retrieved from the ovaries, and joined with sperm in vitro (in the laboratory), in order to obtain embryos that are later transferred inside the mother's uterus to achieve a pregnancy.
IVF is currently the main treatment for infertility, and is indicated in many scenarios:
An IVF cycle requires approximately between 12 and 20 days from start to finish, and includes several steps.
Controlled Ovarian Stimulation (COS) allows to obtain multiple mature oocytes, instead of the single oocyte that ovulates in a normal cycle, in order to increase the chances of pregnancy. It starts with an ultrasound performed on the first or second day of the menstrual cycle to confirm the number of follicles and rule out any cysts.
Daily subcutaneous injections of gonadotropins are then started. These injections are patient friendly and can be performed by the woman or her partner at home, or by a nurse or the local pharmacist. The type and dose of gonadotropins, as well as the COS protocol, are chosen by the physician based on several elements such as age and ovarian reserve.
During COS, the patient needs several visits to the doctor's office (3 to 4 on average), where she undergoes a pelvic ultrasound and a blood test to monitor the response to stimulation (follicular growth and endometrial thickness). When the tests confirm that the follicles are ready (3 or more with a diameter of 17 to 18 mm), an ovulation injection is prescribed (usually hCG), and the oocyte retrieval is scheduled 36 hours later.
The oocyte retrieval is the procedure that allows to recover the mature oocytes from the ovaries. It is performed in the operating theater of the IVF laboratory, and usually requires 15 to 20 minutes. It is performed under light sedation, so the patient should be fasting from midnight of the previous day.
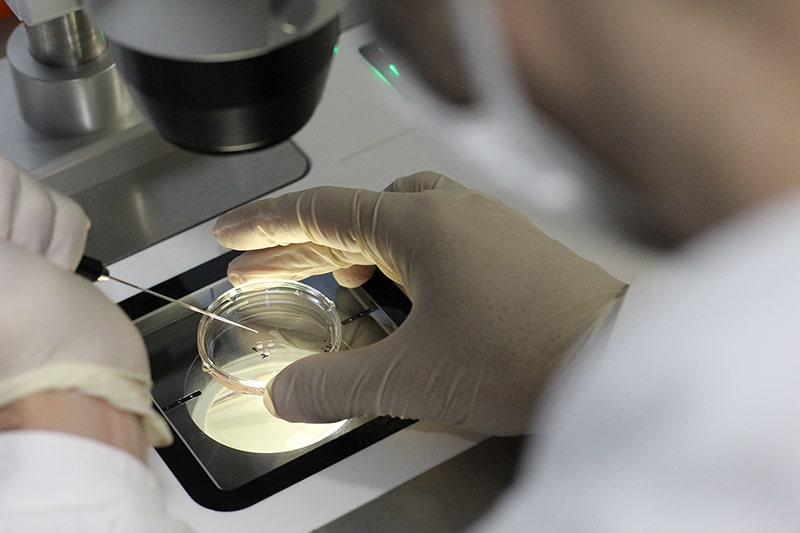
The retrieval is done through the vagina, under ultrasound guidance, using a specific needle to aspirate the fluid from all the follicles. The fluid is immediately passed to the laboratory to isolate the oocytes and prepare them for fertilization.
After the retrieval, the patient rests in the recovery room for about an hour before being discharged home, and she can resume her everyday activity the following day. The partner gives the sperm on the day of the oocyte retrieval, following a period of abstinence of 2 to 5 days.
This step is the cornerstone of the cycle. In vitro (in the laboratory), the sperm fertilizes the mature oocyte to produce an embryo. There are two techniques of in vitro fertilization:

The physician and the embryologist will take several factors into consideration (cause of infertility, quality of sperm, etc.) when deciding which of these two techniques to use. On the following day, the fertilization is checked. Each fertilized egg is now considered an embryo.
Following fertilization, the embryos are placed in small dishes containing culture media to allow them to divide and develop normally. The dishes are placed in incubators that control the environment (temperature, atmospheric pressure, etc.) and keep it suitable for the embryos to grow.

Embryos are kept in culture for a period of 3 to 6 days, during which they are periodically monitored by the embryologists. Several factors are taken into account when assessing the quality of an embryo: the number of cells, the fragmentation, the morphology, and the speed of division.
It is important to note that not all oocytes will be fertilized, and not all embryos will develop normally. The best embryos will be chosen to be transferred and cryopreserved, while the poor quality embryos will stop developing and be discarded.
Embryos can be transferred back to the uterus on day 3, 5 or 6 after the retrieval. The main condition is that the endometrial lining (inner layer of the uterus) is adequate (thickness and appearance), which is confirmed by a pelvic ultrasound.
The transfer is performed at the IVF laboratory as an outpatient procedure. It is painless, does not require any anesthesia, and takes approximately 10 minutes. With the patient lying in the supine position, a transfer catheter is gently inserted into the uterus, under ultrasound guidance. Once the catheter is confirmed to be in the right place inside the uterus, the embryos are loaded into the catheter and transferred into the uterus. The patient remains lying for 30 to 45 minutes after the transfer, and is discharged immediately after.
The decision on the number of embryos and the day of transfer is made by the treating physician and the embryologist, based on many clinical factors (age, history of previous treatments, type and duration of infertility) and biological factors (number and quality of embryos, endometrial thickness).
Nowadays, the gold standard is the transfer of a single blastocyst (Day 5 embryo). Extended culture to the blastocyst stage allows for the selection of the embryos with the highest implantation potential, and the transfer of a single embryo allows to reduce the risk of multiple pregnancies.
The luteal phase refers to the period of time between the oocyte retrieval and the pregnancy test. It is a crucial period for the implantation of the embryo and the achievement of a healthy pregnancy. Progesterone is always added during the luteal phase to support the embryo implantation. Depending on the case, other medications could be added. The patient may resume normal daily activity during that period, although it is better to avoid high intensity activities.
The pregnancy test is usually performed 9 to 12 days after the embryo transfer. A blood test (quantitative bHCG measurement) should be performed, regardless of the patient's symptoms. A positive test is usually repeated after 48 hours to confirm the evolution of the pregnancy. The patient with a positive test should contact her treating physician for next steps. The first ultrasound to confirm the pregnancy is usually performed two to three weeks after the positive test.
For couples who have many good quality embryos, it is recommended to cryopreserve (freeze) the extra embryos that were not transferred. These extra embryos provide further opportunities for future pregnancies without going through the whole IVF process.

Embryos are cryopreserved by vitrification, an ultra-rapid freezing method, and stored in liquid nitrogen at -196 °C. Once frozen, the embryos can be stored indefinitely, without any alteration in their quality.
Frozen embryo transfer (FET) is now an integral part of infertility treatments. It allows couples to have multiple embryo transfers without the need for multiple ovarian stimulations and oocyte retrievals, increasing their chances of pregnancies and of having many babies. In experienced centers, embryos frozen by vitrification offer the same pregnancy rates as fresh embryos. The safety of embryo vitrification has been confirmed, with no health risks for the babies born from vitrified embryos.
IVF is associated with a relatively low rate of complications, most of them minor. The major complication of IVF is Ovarian Hyperstimulation Syndrome (OHSS).
The gonadotropins injected during COS can cause mild bruising or temporary allergic reaction at the injection site, abdominal bloating, breast tenderness, nausea, fatigue, mood swings, and increased vaginal discharge. In general, all these symptoms are minor and do not lead to discontinuation of the treatment.
Mild to moderate abdominal and pelvic pain during the procedure or for a couple of days after, light vaginal bleeding (spotting), and very rarely, injury to organs adjacent to the ovaries or pelvic infection.
Abdominal cramps during or immediately after the transfer. Pelvic infection in extremely rare cases.
Abdominal cramps and bloating, breast tenderness, fatigue, mood swings, and constipation. Ovarian torsion can occur in extremely rare cases and causes severe abdominal pain.
In general, pregnancies obtained by IVF are not considered at higher risk than spontaneous pregnancies. Possible complications include pregnancy loss (miscarriage), ectopic pregnancy, and multiple pregnancies. The Single Embryo Transfer on Day 5 policy significantly decreases the rate of multiple pregnancies.
OHSS is an excessive response of the ovaries to controlled ovarian stimulation, and is the most serious complication associated with IVF. Risk factors include young age, polycystic ovarian syndrome, high ovarian reserve, low body weight, large number of growing follicles and high estradiol levels, high gonadotropin doses, and previous history of OHSS.
OHSS is successfully prevented today with careful screening of patients at risk, individualized treatment plans, the antagonist protocol with GnRH agonist trigger in women at risk, and embryo freezing with cancellation of the embryo transfer when needed.
When you are ready to explore your options, we are here for you. Our fertility experts will help craft a personalized plan based on your needs.
We will get back to you within 24 hours.